
Menopause and Weight Gain: Why It Happens and What GLP-1 Therapy Addresses
EllieMD
Menopausal weight gain is not about eating more. It is about metabolic changes driven by estrogen loss. Here is what is actually happening and why GLP-1 therapy is one of the most effective tools available.
Women consistently describe menopausal weight gain as one of the most frustrating health changes they experience, and a significant part of the frustration comes from being told that the solution is simply eating less and exercising more, as if the change in their body were purely behavioral. The biology tells a more complicated story, and understanding it is the first step toward addressing it effectively.
What Estrogen Does for Weight Regulation
Estrogen is not primarily a reproductive hormone in terms of its systemic effects. It is a broad regulatory molecule with receptors in fat tissue, muscle, liver, bone, brain, and the cardiovascular system. For weight regulation specifically, estrogen does several things that its decline unmakes.
Estrogen promotes the preferential storage of fat in peripheral depots, particularly subcutaneous fat in the hips and thighs, rather than visceral fat around the organs. Visceral fat is metabolically active in ways that subcutaneous fat is not: it secretes inflammatory cytokines, disrupts insulin signaling, and is more strongly associated with cardiovascular and metabolic disease risk. The shift from peripheral to central fat distribution that accompanies estrogen decline is not just a cosmetic change. It is a meaningful metabolic risk shift.
Estrogen supports insulin sensitivity in muscle and other metabolic tissues. As estrogen declines, insulin resistance increases, and the same caloric intake that previously maintained weight begins to produce weight gain as the metabolic machinery becomes less efficient.
Estrogen influences the activity of hypothalamic neurons that regulate appetite and energy expenditure. Its decline changes the set point at which the body defends its weight, making it harder to maintain a lower weight and easier to gain.
Estrogen affects the distribution of muscle versus fat mass. As it declines, muscle is replaced by fat even at a stable body weight in some women, producing a body composition change that is invisible on the scale but clinically significant.
Why Previous Approaches Stop Working
Many women who managed their weight successfully through their 30s and early 40s find that the same dietary patterns and exercise routines stop working during the menopausal transition. This is not imaginary and it is not a motivation problem. It is a metabolic environment change that made the previous approach insufficient.
The caloric requirement for weight maintenance decreases during the menopausal transition as muscle mass shifts to fat and metabolic rate changes. Simultaneously, appetite may increase due to the hypothalamic changes that estrogen decline drives. The combination produces genuine weight gain at a caloric intake that was previously maintenance.
Telling women in this situation to simply try harder with approaches that are biologically less effective than they were before is not useful clinical advice.
Where GLP-1 Therapy Addresses the Problem
GLP-1 therapy for menopausal weight gain addresses several of the biological mechanisms directly.
The insulin resistance that estrogen decline produces is improved by GLP-1 receptor agonism, which enhances glucose-dependent insulin secretion and improves peripheral insulin sensitivity. For women whose menopausal weight gain is partly driven by the metabolic consequences of worsening insulin sensitivity, this is a targeted mechanism.
The visceral fat accumulation that accompanies the loss of estrogen's fat distribution regulation is specifically the type of fat that GLP-1 therapy is most effective at reducing. Central adiposity is more responsive to the metabolic and appetite effects of GLP-1 therapy than peripheral subcutaneous fat.
The appetite changes driven by hypothalamic shifts during menopause are modulated by GLP-1 receptor activation in the same hypothalamic regions, which helps recalibrate the appetite set point that estrogen loss has disrupted.
The Broader Longevity Picture
For women navigating the menopausal transition, GLP-1 therapy is most effective as one component of a comprehensive approach that acknowledges what the biology of the transition demands. Resistance training is more important during this period than before it, specifically to counteract the muscle mass loss that accompanies estrogen decline. Sleep quality directly affects the cortisol and metabolic picture. Stress management affects the hormonal balance in ways that compound the estrogen-related changes.
EllieMD's longevity and weight loss programs can be coordinated for women navigating the menopausal transition. Your physician consultation is where the intersection of these factors is addressed as a clinical whole rather than as separate isolated issues.
Individual results may vary. All prescriptions require approval by a licensed medical provider. Compounded medications are not FDA-approved. EllieMD facilitates access to independent healthcare providers and pharmacies and does not provide medical care or dispense medications.
Related Articles
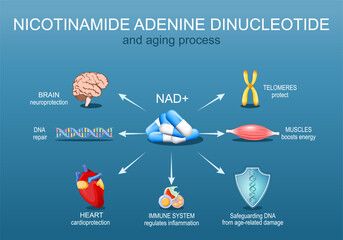
NAD+ Oral Drops with GLP-1: What the Combined Formulation Is Designed to Do
EllieMD

GLP-1 and Joint Pain: The Connection Between Weight, Inflammation, and Chronic Pain
EllieMD

GLP-1 Side Effects: What to Expect and How to Manage Them
EllieMD
GLP-1 and Testosterone: What Men Need to Know About the Hormonal Connection
EllieMD

How Does GLP-1 Work in the Body? A Plain-Language Explanation
EllieMD

The Science of Appetite: Why Hunger Is Hormonal, Not a Character Flaw
EllieMD
Get the latest updates and exclusive offers by subscribing to our newsletter.
© 2026 EllieMD LLC. All rights reserved.