
Intermittent Fasting and GLP-1: Do They Work Together?
EllieMD
Intermittent fasting and GLP-1 therapy both affect appetite and metabolic function. Here is what happens when you combine them and how to think about whether it makes sense for you.
Intermittent fasting has been one of the most widely adopted dietary frameworks of the past decade, and many people who start GLP-1 therapy are already practicing some form of time-restricted eating. The question of whether the two approaches work together, work against each other, or simply stack on top of each other without meaningful interaction is worth examining carefully.
The short answer is that they can work well together for some patients and create problems for others, and the determining factors are not the same for everyone.
How Each Approach Works IndependentlyIntermittent fasting encompasses a range of protocols, the most common being a 16:8 pattern (16 hours fasting, 8 hours eating window), alternate day fasting, and the 5:2 protocol (normal eating five days, significant restriction two days per week). The common thread is a structured restriction of the eating window rather than specific caloric or macronutrient targets.
The proposed mechanisms of intermittent fasting for metabolic health include improved insulin sensitivity, reduced overall caloric intake through the shortened eating window, activation of autophagy during fasting periods, and in some research, direct metabolic effects independent of caloric restriction.
GLP-1 therapy works through appetite suppression via central nervous system receptor activation, slowed gastric emptying, improved glucose-dependent insulin secretion, and several downstream metabolic effects. The appetite reduction is the primary driver of the caloric deficit that produces weight loss.
Where They OverlapBoth approaches reduce caloric intake. Both improve insulin sensitivity. Both have been associated with improvements in body weight and metabolic markers. In this sense, combining them is not pharmacologically contradictory.
For patients already practicing intermittent fasting who then add GLP-1 therapy, the two approaches often reinforce each other in the short term. The appetite suppression from GLP-1 makes adhering to a restricted eating window easier, because the drive to eat during the fasting period is already reduced. Patients who previously found 16:8 difficult because of hunger during the fasting window often find it effortless on GLP-1 therapy.
Where Combination Can Become ProblematicThe issue is not the combination itself but the degree of caloric restriction it can produce when both work simultaneously and when adequate nutrition is not prioritized.
GLP-1 therapy already produces significant reduction in total caloric intake. Intermittent fasting further compresses the window in which food is consumed. If the eating window is too short and the appetite suppression too strong, the result can be inadequate total food intake, particularly inadequate protein, which compromises lean mass preservation and can produce nutritional deficiencies over time.
Patients who are already eating very little on GLP-1 therapy and then try to fit that reduced intake into a 6 to 8 hour window may find they simply cannot consume adequate nutrition in that timeframe, particularly if nausea is present.
There is also a practical concern about energy levels and medication tolerability. Some patients taking GLP-1 medications on an extended fasting state find that GI side effects, particularly nausea, are worse without any food in the system.
The Practical ApproachIf you are currently practicing intermittent fasting and starting GLP-1 therapy, the sensible approach is to start the medication without making changes to your eating pattern, observe how your appetite and tolerability evolve over the first few weeks, and then assess whether your food intake within the eating window is adequate in terms of total nutrition and particularly protein.
If you are on GLP-1 therapy and considering adding intermittent fasting, discuss it with your physician before implementing. The key question is whether your current caloric and protein intake is already at the lower limit of what supports lean mass preservation. If it is, adding an eating window restriction without deliberate nutritional management is likely to compromise your body composition outcomes.
Time-restricted eating for its own metabolic benefits makes sense for some patients on GLP-1 therapy. It should be implemented thoughtfully rather than as a default intensification of an already significant caloric restriction.
Individual results may vary. All prescriptions require approval by a licensed medical provider. Compounded medications are not FDA-approved. EllieMD facilitates access to independent healthcare providers and pharmacies and does not provide medical care or dispense medications.
Related Articles
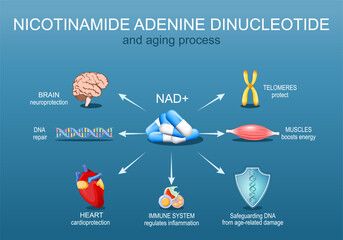
NAD+ Oral Drops with GLP-1: What the Combined Formulation Is Designed to Do
EllieMD

GLP-1 and Joint Pain: The Connection Between Weight, Inflammation, and Chronic Pain
EllieMD

GLP-1 Side Effects: What to Expect and How to Manage Them
EllieMD
GLP-1 and Testosterone: What Men Need to Know About the Hormonal Connection
EllieMD

How Does GLP-1 Work in the Body? A Plain-Language Explanation
EllieMD

The Science of Appetite: Why Hunger Is Hormonal, Not a Character Flaw
EllieMD
Get the latest updates and exclusive offers by subscribing to our newsletter.
© 2026 EllieMD LLC. All rights reserved.