GLP-1 and Fatty Liver Disease: What the Research Shows
EllieMD
Non-alcoholic fatty liver disease affects roughly a third of American adults and is closely tied to metabolic dysfunction. Here is what GLP-1 therapy does to liver fat and why it matters.
Non-alcoholic fatty liver disease, now more precisely called metabolic dysfunction-associated steatotic liver disease (MASLD), is one of the most common chronic conditions in the United States. It affects an estimated 80 to 100 million Americans and is strongly associated with obesity, insulin resistance, and type 2 diabetes. For a significant portion of patients starting GLP-1 therapy for weight loss or metabolic health, MASLD is either already present or developing silently.
Understanding how GLP-1 therapy affects the liver adds a meaningful dimension to what these medications are doing for your health, beyond the appetite and scale changes.
What Fatty Liver Disease Actually Is
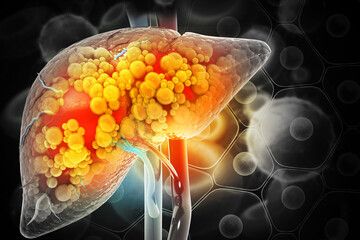
The liver is the body's primary metabolic processing center. Under normal conditions, it handles fat metabolism, glucose storage and release, protein synthesis, and detoxification. When the metabolic load becomes too great, particularly in the context of chronic insulin resistance and excess caloric intake, the liver begins accumulating fat in its cells in amounts that exceed what normal liver tissue contains.
This fat accumulation, called hepatic steatosis, is the defining feature of MASLD. In its early stages it is largely asymptomatic. The liver has no pain receptors, so fat accumulation does not produce the warning signal that other organ stress does. Many people have significant hepatic steatosis discovered incidentally on an abdominal ultrasound done for a different reason.
The clinical concern is progression. In roughly 10 to 20 percent of people with simple steatosis, the condition progresses to metabolic-associated steatohepatitis (MASH), in which liver cell inflammation and damage accompany the fat accumulation. Continued progression leads to fibrosis, then cirrhosis, and in some cases liver failure or hepatocellular carcinoma. MASLD has become one of the leading indications for liver transplant in the United States.
The driver of both the initial fat accumulation and the progression to inflammation is the same metabolic dysfunction that drives obesity, insulin resistance, and cardiovascular disease. Visceral fat releases fatty acids into the portal circulation, which goes directly to the liver. Insulin resistance in the liver disrupts normal fat metabolism. The liver accumulates fat as a consequence of the same systemic metabolic problem that is driving weight gain.
What GLP-1 Therapy Does to Liver Fat
GLP-1 receptor agonists reduce liver fat through two distinct pathways that work simultaneously.
The first is indirect, through weight loss and improved insulin sensitivity. Reducing body weight, particularly visceral fat, reduces the delivery of free fatty acids to the liver through the portal circulation. Improving insulin sensitivity reduces the hepatic fat synthesis that insulin resistance promotes. Studies consistently show that weight loss of 7 to 10 percent of body weight produces measurable reduction in liver fat content regardless of how the weight loss is achieved.
The second pathway is more direct. GLP-1 receptors are expressed in the liver, and their activation appears to reduce hepatic fat synthesis and promote fat oxidation through mechanisms independent of weight loss. This direct hepatic effect is supported by research showing that GLP-1 receptor agonists reduce liver fat content to a greater degree than would be expected from weight loss alone.
A landmark trial published in the New England Journal of Medicine in 2021, the NASH trial of semaglutide, found that semaglutide produced resolution of MASH without worsening of fibrosis in 59 percent of participants compared to 17 percent in the placebo group. This was in patients with confirmed MASH on biopsy, the more advanced inflammatory stage. The result was significant enough that the FDA approved semaglutide for MASH in 2024, making it the first approved treatment specifically for this condition.
Why This Matters Beyond the Scale
For many patients starting GLP-1 therapy primarily for weight loss, the liver fat reduction happening in parallel is not visible on the scale or in the mirror, but it may be the most clinically significant change occurring.
MASLD at the steatohepatitis stage accelerates cardiovascular risk, impairs glucose metabolism, and if it progresses to fibrosis, becomes an independent driver of serious health complications that are difficult to reverse. Addressing it during the steatosis or early steatohepatitis phase, before fibrosis establishes itself, is the window in which intervention is most effective.
If you have been told you have fatty liver, elevated liver enzymes, or MASLD on imaging, this is a relevant dimension of your GLP-1 consultation to raise explicitly. Your EllieMD physician can factor it into the clinical picture and help you track whether liver markers are improving alongside the other outcomes you are measuring.
Individual results may vary. All prescriptions require approval by a licensed medical provider. Compounded medications are not FDA-approved. EllieMD facilitates access to independent healthcare providers and pharmacies and does not provide medical care or dispense medications.
Related Articles
NAD+ Oral Drops with GLP-1: What the Combined Formulation Is Designed to Do
EllieMD

GLP-1 and Joint Pain: The Connection Between Weight, Inflammation, and Chronic Pain
EllieMD

GLP-1 Side Effects: What to Expect and How to Manage Them
EllieMD
GLP-1 and Testosterone: What Men Need to Know About the Hormonal Connection
EllieMD

How Does GLP-1 Work in the Body? A Plain-Language Explanation
EllieMD

The Science of Appetite: Why Hunger Is Hormonal, Not a Character Flaw
EllieMD
Get the latest updates and exclusive offers by subscribing to our newsletter.
© 2026 EllieMD LLC. All rights reserved.